When Hauwa (not her real name), a 28-year-old mother of four in Abuja, described how she tries to prevent pregnancy, she mentioned a home practice recommended by neighbours and older women. “After my last child, I was told to rinse with salt water to avoid getting pregnant again.” Similar anecdotes are . While these practices are culturally entrenched, there is no scientific evidence that they prevent pregnancy and can sometimes pose health risks. Yet, they persist, pointing to a deeper problem: the gap between knowledge, access, and women’s reproductive autonomy.
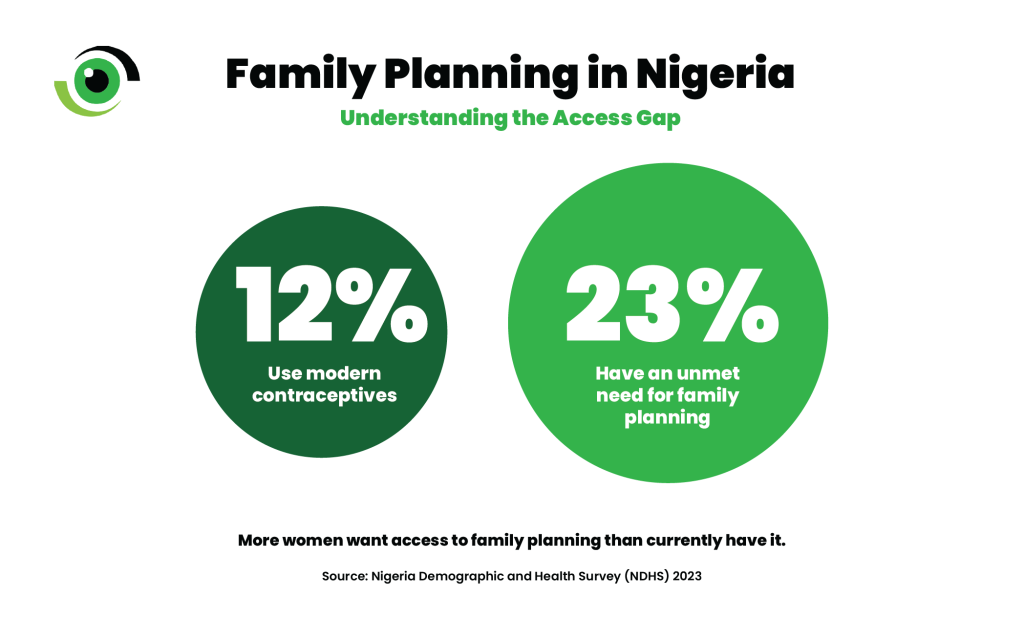
More than a health intervention, family planning is a , economic opportunity, and societal wellbeing. Yet Nigeria’s modern contraceptive prevalence . The country’s modern contraceptive prevalence rate (mCPR) , one of the lowest globally and far below of 60%, or 80% to 90% in some high-income countries. These figures represent millions of women whose reproductive choices are constrained by misinformation, systemic barriers, and socio-cultural norms.
The roots of misconceptions
Traditional practices often shared through family and peer networks remain common in many Nigerian communities. are sometimes seen as “safer” or “more natural” than modern contraceptive methods, shaped by cultural norms, community trust, and distrust of formal health services., family planning services can be distant, costly once transport and time are counted, and surrounded by stigma for women who try to use them. It also helps to separate myths from such as , which require accurate information and consistent use to be effective.
Even when services are available, , worries about future fertility, and poor counselling can deter women from choosing medically approved options. These practices are not simply about ignorance. They reflect trust in tradition, social reinforcement, and limited access to accurate information. As Nafisa (not her real name), a resident of Wassa IDP camp in Abuja explained, “women here want to space their children, but we fear pills and injections. We rely on what our mothers and neighbours taught us.” This highlights that contraceptive uptake is intertwined with empowerment, trust, and informed decision-making.
Health workers warn that many of these home practices have no scientific basis for preventing pregnancy and may carry health risks. Dr Farida Adeyemo, a medical doctor at Deda Hospital, said: “Salt water and herbal mixtures do not prevent pregnancy. Some practices can also irritate or injure the reproductive tract.” She further noted that myths about contraceptives, particularly fears of infertility, contribute significantly to low uptake. She explained that side effects vary by method and that counselling changes everything. “For example, some women experience heavier bleeding with a copper IUD, especially at first. If women know what to expect and when to return for support, they are more likely to continue or switch safely.” She emphasised that follow-up is critical because, “we may not get it right the first time. That’s why method switching is common if side effects are not tolerable.”
Expanding proven models in Nigeria
Evidence from Nigeria and across Africa demonstrates that well-supported contraceptive programmes can overcome mistrust. A in two rural communities in Ebonyi State implemented community mobilisation activities, engaging local leaders and distributing Information, Education, and Communication (IEC) materials. Awareness of family planning among women increased from , and uptake of family planning rose from over the intervention period. This shows how culturally grounded, community‑led engagement can shift both knowledge and behaviour around contraception, helping to dismantle myths.
In Kano State, engaged both men and women in discussions about child spacing and contraceptive use, raising awareness and increasing access to family planning services across communities. led to higher awareness, greater adoption of contraceptives, and more informed, joint reproductive decisions. A in Lagos assessed whether pharmacies and patent and proprietary medicine vendors (PPMVs) followed the Ministry of Health guidance when dispensing the (DMPA‑SC) for self-injection.
The findings revealed that many vendors, particularly in private outlets, did not provide clients with proper instructions or counselling. This highlights the need for stronger quality assurance measures in pharmacies and PPMVs, ensuring women receive safe and accurate guidance, an essential step for building trust and supporting the successful adoption of self-care contraceptive methods. While self‑care has strong potential, safe scale-up depends on consistent, client-centred counselling, clear referral pathways, and follow-up support.
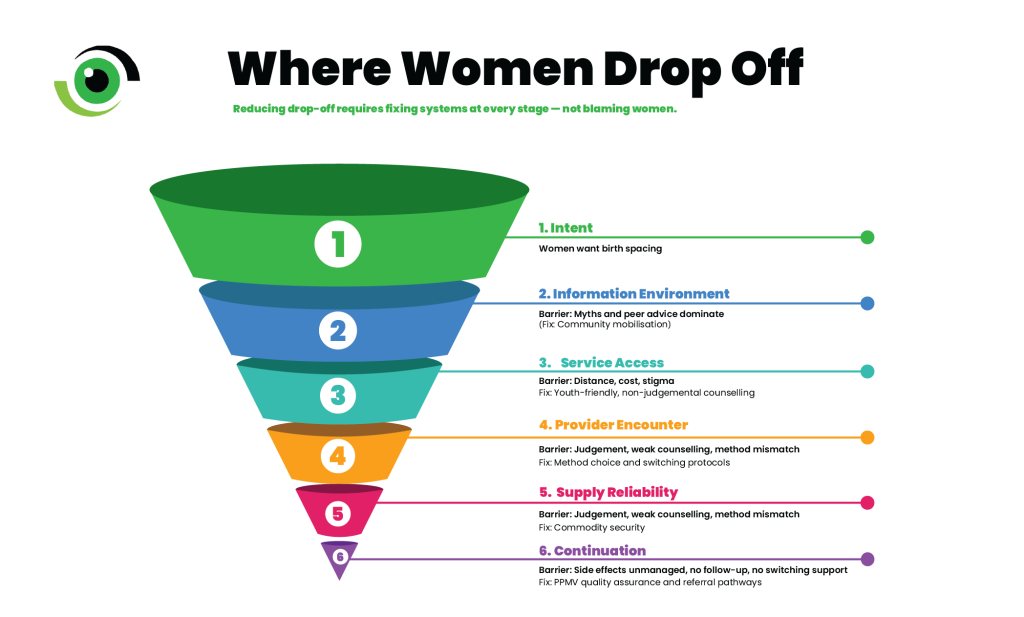
Improving family planning in Nigeria is not only about supplying modern contraceptive commodities. It is about trust, accurate information, respectful care, and women’s ability to choose freely. When counselling is weak and services feel judgemental or unreliable, myths fill the gap. The next step for policymakers and key decision makers to fund and implement , invest in community-led demand generation, strengthen commodity security, train providers to offer non-judgemental counselling, including for adolescents, and regulate and support PPMVs to deliver quality guidance, especially as self-care expands.